
Anatomic Relationship between the Impacted Mandibular
Canine and the Mental Nerve: A Case Report
Shivendra Singh1
, Meghna Kumar2
, Nishant Singh3
, Ankit Singla4
, Gaurav Rai5
, Kirti Prakash6
1
Assistant Professor, Department of Oral and Maxillofacial Surgery, Rama Dental College, Hospital and Research Centre,
Kanpur, 2
Post-Graduate Student, Department of Oral and Maxillofacial Surgery, Rama Dental College, Hospital and Research
Centre, Kanpur, 3
Professor, Department of Oral and Maxillofacial Surgery, Rama Dental College, Hospital and Research
Centre, Kanpur, 4
Post-Graduate Student, Department of Oral and Maxillofacial Surgery, Rama Dental College, Hospital and
Research Centre, Kanpur, 5
Post-Graduate Student, Department of Oral and Maxillofacial Surgery, Rama Dental College,
Hospital and Research Centre, Kanpur, 6
Post-Graduate Student, Department of Oral and Maxillofacial Surgery, Rama Dental
College, Hospital and Research Centre, Kanpur, India
Corresponding author: Dr Meghna Kumar (MDS), Post-Graduate Student, Department of Oral and Maxillofacial Surgery,
Rama Dental College, Hospital and Research Centre, Kanpur, India
DOI: http://dx.doi.org/10.21276/ijcmsr.2020.5.1.14
How to cite this article: Shivendra Singh, Meghna Kumar, Nishant Singh, Ankit Singla¸ Gaurav Rai¸ Kirti
Prakash. Anatomic relationship between the impacted mandibular canine and the mental nerve: a case report.
International Journal of Contemporary Medicine Surgery and Radiology. 2020;5(1):A56-A58.
Introduction:
Impacted teeth can be defined asthose that do not erupt at the normal age of eruption and remain embedded
in the maxilla or mandible where they are either partially or completely surrounded by bone or soft tissues. Clinically,
impacted teeth are seen in about 20% of the population. Third molars are the most commonly impacted teeth, followed by
the maxillary canines and the mandibular bicuspids.
Case report: A 55-year old male reported to the Department of Oral and Maxillofacial Surgery, Rama Dental College;
complaining of pain and swelling in the lower left anterior region of the jaw since 1 week. An ortho-pantomogram of the
patient revealed an impacted distoangular 33, at Level C with respect to 34. The patient was prescribed oral antibiotics and
analgesics for three days to alleviate pain and swelling. The impacted tooth(33) was then surgically extracted under local
anesthesia. The mental foramen was located apical to 34. The patient was recalled after a week for suture removal. The
healing was uneventful. No paresthesia of the left side of lower lip, left gingiva or left buccal mucosa was observed.
Conclusion: This case report emphasizesthe need for careful radiographic assessment of the mandibular canal and foramina
pre-operatively and careful sub-periosteal dissection to avoid inadvertent damage to the mental nerve during extraction of
impacted mandibular canine leading to paresthesia of the lower lip, mandibular labial gingiva and chin.
INTRODUCTION
Impacted teeth can be defined as those that have not
erupted into occlusion according to chronological age due
to obstruction by bone or soft tissue. Impaction of teeth is
clinically seen commonly in about 20% of the population.1
The frequency of impaction in Mongoloid races has been
found to be 2.5 times more than in Caucasians.2
Third
molars are the most commonly impacted teeth(mainly in the
mandible) followed by maxillary canines and the mandibular
premolars.3
Impacted teeth must be diagnosed and treated
promptly, as they may lead to formation of pathological cysts.
Impaction of maxillary canines has an incidence of between
0.8 to 2.3%.4
The occurrence of impaction and/or noneruption of mandibular canines is unusual, with prevalence
rates from 0.05 to 0.4%.5
Several etiological factors have been
linked with the impaction of a mandibular canine, such as
an eruption disturbance caused by an anomaly of the canine
germ itself.6
Trauma, pathological conditions (odontomes,
cyst), crowding, and early loss of primary canines and
mandibular fractures may also be a causative factor.7
Often, impacted teeth may be retained while still
asymptomatic.8
However, Bishara et al. suggested the
following sequelae of canine impaction9,10:
• Movement of the impacted tooth to a labial or lingual
position
• Migration of the adjacent teeth and reduction in arch
length
• Root resorption of the impacted tooth as well as the
adjacent teeth
• Inflammation associated with partial eruption causing
pain and trismus
• Pain radiation to the temporo-mandibular jaw or the
temporal region
The mental nerve, arising from the mental foramen present
in the canine-premolar region provides sensory innervation
to the chin, labial gingival and lower lip. Therefore, the
nerve should be isolated and protected during all surgical.
Initial examination: A 55-year old male reported to the
Department of Oral and Maxillofacial Surgery, Rama
Dental College, complaining of pain and swelling in
the lower left anterior region of the jaw since 1 week.
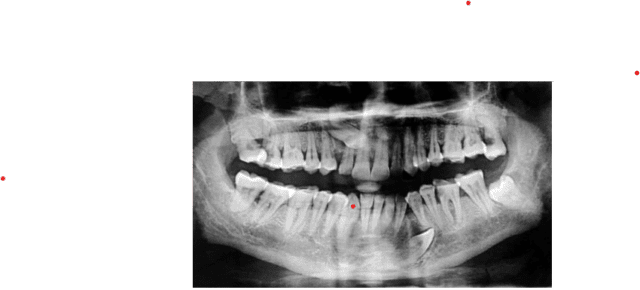
tooth to be an impacted 33 at Level C with respect to 34

vestibular incision extending from 41 to 35


ortho-pantomogram of the patient revealed an impacted
distoangular 33, at Level C with respect to 34 (Image 1).
No significant medical history was found, and no other
extraoral or intraoral abnormality was detected.The patient
was prescribed antibiotics and analgesics to alleviate the
symptoms, and was recalled after two days.
Treatment:
The patient was prepared and draped according
to standard protocol. The inferior alveolar nerve block and the
lingual nerve block was administered bilaterally.
Additionally,
an infiltration nerve block was given between 32 and 35 to
minimize bleeding at the operation site.
A vestibular degloving incision was given extending from
41 to 35. Careful sub-periosteal dissection was done both
superiorly and inferiorly to expose the crown of 33 and the
inferior border of the mandible respectively, while preserving
the mental nerve (Image 2).
The mental foramen was located
apical to 34 (Image 3). A stainless steel round bur was used
to completely expose the crown of the impacted canine and
the root up to its upper one third (Image 4). The crown was
sectioned using a no.702 stainless steel bur.
The crown and
root were then removed separately.
The bony socket was irrigated with 5% betadine solution
and the defect was closed with simple, interrupted
sutures using 3-0 silk.
A pressure dressing with gauze and
dynaplast was applied and the patient was prescribed a
course of Amoxicillin+Potassium Clavulanate (625mg)
TID, Metronidazole (400mg) TID, Aceclofenac +
Serratiopeptidase + Paracetamol (100mg+15mg+325mg)
BD, and Pantoprazole (40mg) OD for 5 days.
Follow-up:
The patient was recalled after seven days for
suture removal. The healing was uneventful. No paresthesia
of the left side of lower lip, left gingiva or left buccal mucosa
was observed.
DISCUSSION
Mandibular canine impaction is considered to be less
common phenomenon than maxillary canine impaction,
and only a few studies recording its frequency can be found
in literature.
16 Grover and Lorton found only 11 impacted
canines (0.22%) in the mandible in 5000 individuals. Chu
et al17 reported five mandibular impacted canine (0.07%)
teeth in 7486 patients.
Rohrer18 examined 3,000 patients and
found 62 impacted maxillary canines (2.06%) as compared to
only three impacted mandibular canines (0.1%).
Multiple etiologies have been described which can lead to
failure of eruption of teeth.
Most surgeons are of the opinion
that these etiologies may include a pathological condition,
inflammation, interference of prosthetic devices, disturbances
of the dentition, pain, and ectopic eruption.
Etiologies specific
to the unerupted mandibular canine include insufficient
space, supernumerary teeth, premature loss of the primary
teeth, retained deciduous canine, excessive crown length,
genetic factors, functional disturbances of the endocrine.
CONCLUSION
The mandibular impacted canine is usually associated in close
proximity with the apex of the mandibular premolars, and
thus the mental nerve and mental foramen.
This case report
emphasizes on the need for careful preoperative radiographic
assessment of the inferior alveolar canal and the mental
foramina followed by careful sub-periosteal dissection to
avoid inadvertent damage to the mental nerve leading to
paresthesia of the lower lip, mandibular labial gingiva and
chin.
Are you searching for the best orthodontists , Visit Dent-O-Face
let know our doctor or go to